CGM Dose Adjustment Calculator
→
Suggested Adjustment
0.0 Units
Total Recommended Dose
0.0 Units
⚠️ Medical Disclaimer: This tool is for educational purposes based on the article's example (CF 1:50). Do not make medication changes without consulting your healthcare provider to determine your specific correction factor and protocol.
Quick Reference (CF 1:50)
| Arrow | Direction | Adult | Pediatric |
|---|---|---|---|
| ⇈ | Fast Rising | +1.2u | +1.0u |
| ↑ | Rising | +0.8u | +0.6u |
| → | Stable | 0 | 0 |
| ↓ | Falling | -0.8u | -0.6u |
| ⇊ | Fast Falling | -1.2u | -1.0u |
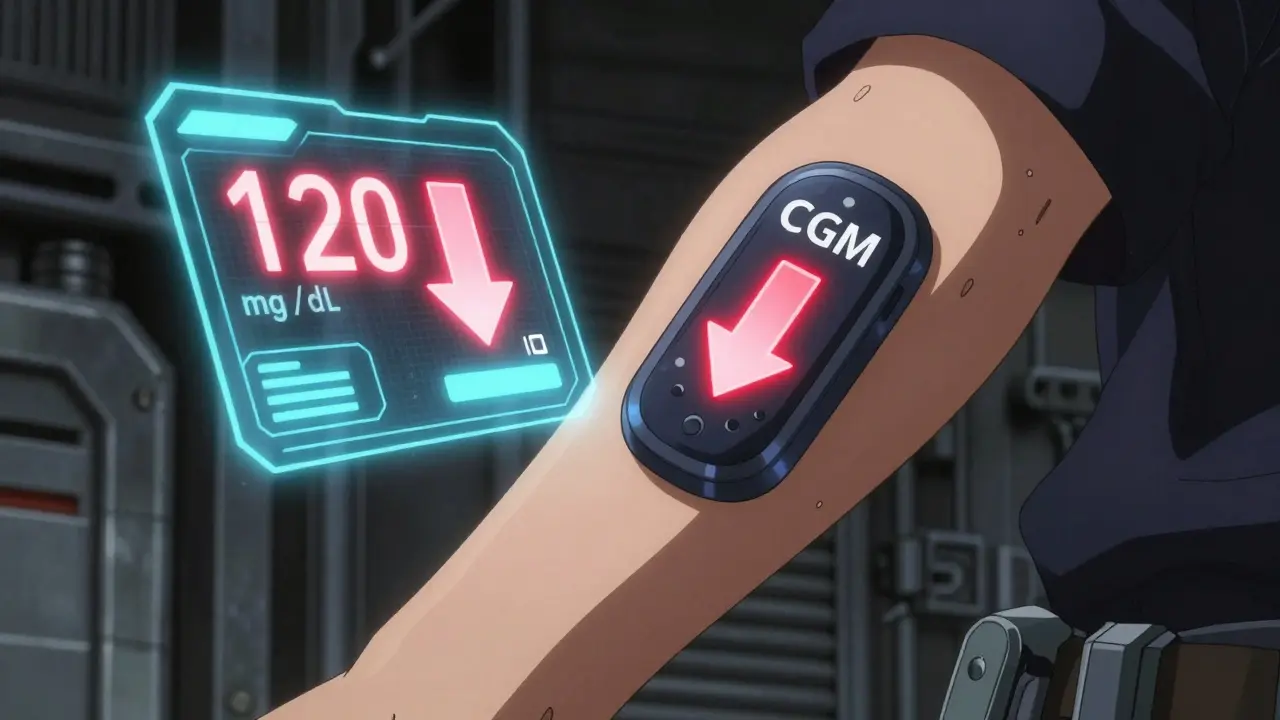
Imagine you're looking at your glucose monitor and you see a number like 120 mg/dL. On paper, that looks perfect. But if there's a double-down arrow next to it, you aren't actually stable-you're crashing. By the time you realize you're low, you might already be shaking or confused. This is the core problem with traditional finger-stick tests; they give you a snapshot of the past, not a map of the future. Continuous Glucose Monitoring is a technology that tracks glucose levels in real-time, providing both current values and directional trend arrows to predict where glucose is heading. Commonly referred to as CGM, these systems allow you to move from reacting to side effects to preventing them before they happen.
Turning Data Into Action with Trend Arrows
Most people use a CGM just to see their current number, but the real magic is in the trend arrows. These arrows tell you the speed and direction of your glucose change. For instance, a "double-up" arrow means your sugar is rising fast, while a "flat" arrow means you're cruising at a steady pace. If you only dose based on the number, you're ignoring the momentum.
To stop the "rollercoaster" effect-where you over-correct a high and plunge into a low-you need a system. The Endocrine Society created standardized protocols specifically for the Dexcom G5 is a professional-grade CGM system that utilizes a subcutaneous sensor to provide glucose readings every five minutes. These guidelines move away from confusing percentages (like "increase dose by 20%") and instead use specific unit adjustments based on your personal sensitivity.
The Math Behind the Adjustment: Correction Factors
Before you can adjust your meds based on an arrow, you have to know your Correction Factor is a value representing how many mg/dL a single unit of insulin lowers a person's blood glucose. For example, if you have a CF of 1:50, one unit of insulin drops your blood sugar by 50 mg/dL. This is the foundation of any dose tweak.
When you combine your CF with the trend arrow, you get a precise instruction. For an adult with a 1:50 CF, the protocol looks like this: if you see a double-up arrow before a meal, you add 1.2 units to your bolus. If you see a double-down arrow, you subtract 1.2 units. It's a simple addition or subtraction that removes the guesswork and prevents the "guessing game" that often leads to severe side effects.
| Trend Arrow | Glucose Direction | Adult Dose Adjustment | Pediatric Dose Adjustment |
|---|---|---|---|
| Double-Up | Fast Rising | +1.2 Units | +1.0 Units |
| Single-Up | Rising | +0.8 Units | +0.6 Units |
| Flat | Stable | No Change | No Change |
| Single-Down | Falling | -0.8 Units | -0.6 Units |
| Double-Down | Fast Falling | -1.2 Units | -1.0 Units |
Preventing Hypoglycemia and Hyperglycemia
The primary "side effects" of insulin aren't like a rash or a headache; they are dangerous glucose excursions. Hypoglycemia is a condition where blood glucose levels drop below 70 mg/dL, potentially causing dizziness, confusion, or loss of consciousness. Conversely, Hyperglycemia is excessively high blood glucose levels that can lead to long-term organ damage or acute ketoacidosis. By adjusting doses based on trend arrows, you're essentially putting a guardrail on both ends of the spectrum.
A study by Peters et al. showed that people using these trend-based adjustments had 28% fewer low-sugar events and spent 17% more time in the target range (70-180 mg/dL) than those using old-school finger sticks. It's the difference between seeing a car crash happen and seeing the car speeding toward the intersection and hitting the brakes in time.
Avoiding the "Over-Correction" Trap
There is a danger here: insulin dose adjustment must be done with an awareness of "insulin on board." If you see a double-up arrow and add extra insulin, but you already have a dose working from an hour ago, you risk "stacking." This happens when multiple doses of insulin overlap, leading to a sudden, massive drop in glucose.
Dr. Irl Hirsch from the University of Washington has pointed out that blindly following arrows without understanding your own insulin kinetics can be risky. About 12% of new CGM users actually increase their risk of lows initially because they over-correct for downward trends. The rule of thumb? Always verify your CGM reading with a finger stick if the arrow seems too aggressive or if you feel different than what the screen is telling you.
Practical Steps for Implementing a Trend-Based Strategy
You can't just start adding units tomorrow morning without a plan. Most endocrinologists suggest a three-step education process to get this right:
- Map Your Timing: Understand when your specific insulin peaks. If you use rapid-acting insulin, it usually hits hardest between 60 and 90 minutes. You need to know this so you don't panic when you see a down arrow shortly after a dose.
- Contextualize the Arrow: Look at your recent history. If you just ate a high-carb snack, a double-up arrow is expected. If you've been sitting still for three hours and see a double-up arrow, that's a different signal entirely.
- Apply the Adjustment: Use the tables provided by your doctor. Start with small changes and keep a log of how your body responds to these tweaks.

Modern Tools and the Future of Dosing
We are moving toward a world where you won't have to do this math manually. The FDA recently cleared apps like DAFNE+ is a CGM-integrated dose adjustment application that automates Endocrine Society calculations to reduce human error. In clinical trials, this automation reduced dosing errors by 62%.
Beyond insulin, these tools are helping with other medications too. For people using SGLT2 inhibitors is a class of medications that lower blood glucose by causing the kidneys to remove sugar from the body through urine. New guidelines suggest reducing these doses if a CGM shows persistent "euglycemic ketosis," where blood sugar looks normal (under 180 mg/dL) but ketones are dangerously high.
Can I use these adjustments with any CGM brand?
While the Endocrine Society guidelines were specifically validated using Dexcom G5 data, the general logic applies to most CGMs. However, be careful: different brands define "fast rising" or "fast falling" differently. For example, Dexcom might trigger a double arrow at a different rate of change than the FreeStyle Libre. Always check your specific device's manual or consult your doctor to ensure the arrow speeds match the adjustment table you're using.
What should I do if the CGM reading and my finger stick don't match?
Trust the finger stick for immediate dosing decisions, especially if you are experiencing symptoms of a high or low. CGMs measure interstitial fluid, not blood, which creates a "lag time" of about 5 to 15 minutes. During rapid glucose changes (indicated by double arrows), this lag is more pronounced. If the two readings differ significantly, use the blood glucose meter value to determine your base dose and the CGM trend arrow to determine if you should slightly increase or decrease that dose.
Is it safe to adjust doses for children using this method?
Yes, but the adjustments are smaller. Because children often have different insulin sensitivities and are more prone to rapid shifts, the pediatric tables recommend smaller unit changes (e.g., +1.0 units for a double-up arrow instead of +1.2). Parents should work closely with a pediatric endocrinologist to set these specific values, as the risk of hypoglycemia can be more acute in children.
What is "trend arrow paralysis"?
This is a common psychological hurdle where a user becomes overwhelmed by the constant stream of data and arrows, leading to an inability to make a dosing decision. It affects about 25% of new users. The best way to overcome this is to stick to a rigid, written protocol (like the Endocrine Society tables) so that the decision is mathematical rather than emotional.
How often should I update my correction factor?
Your correction factor can change due to age, weight loss, illness, or changes in other medications. You should review your CF with your provider every 3-6 months or whenever you notice a consistent pattern of over-shooting or under-shooting your target glucose levels despite following the trend arrow adjustments.
Next Steps and Troubleshooting
If you're just starting out, don't try to master every arrow at once. Start by observing your patterns for one week without making changes. Notice how often you see double-down arrows before a crash. Once you recognize the pattern, introduce adjustments for only one type of arrow-perhaps the "fast falling" ones-to prevent lows.
If you find that you're still experiencing frequent lows despite adjusting downward, you may have "insulin stacking." Check your logs to see if you're dosing corrections too close together (less than 3-4 hours apart). In these cases, the trend arrow is telling you the truth, but your body is still processing the previous dose. When in doubt, prioritize safety over a perfect number and opt for a smaller dose or a snack.